

Past Projects
REFUGE-ED
Project Title: REFUGE-ED - Effective practices in education, mental health and psychosocial support for the integration of refugee children
Summary: REFUGE-ED seeks to develop a Brokering Knowledge Platform of Effective Practices (BKP), which will host and promote education as well as mental health and psychosocial support solutions for the integration of migrant and refugee children in schools and more broadly in society. A process of co-creation - using a dialogic process with children, families, teachers, practitioners working on the ground, policy-makers and other relevant stakeholders, and applying a new communicative methodology developed by the consortium (SPICE) - will be applied to co-create knowledge and identify pilot actions to be carried out across multiple sites, including hot spots/reception identification centres, inclusive school environments and non-formal and informal social and learning environments, and institutional care (including unaccompanied minors). In total, the REFUGE-ED project has carried out multisite pilot actions across 6 countries (Sweden, Ireland, Spain, Italy, Greece and Bulgaria). The final co-created BKP will provide tools, solutions and recommendations, including guidelines and criteria on capacity building training, solution adaptation and community engagement in easy-to-use off-line package, in different formats, to support the implementation, reuse and scalability of the piloted actions, and of other practices identified as successful.
Partners: Autonomous University of Barcelona (AUB; Lead Coordinator); University of Florence; New Bulgarian University; Kentro Merimnas Oikogeneias Kai Paidiou (Family & Childcare Centre; KMOP), Save the Children Denmark, Danish Red Cross, Support Group Network, Associazione Culturale Cooperazione Internazionale Sud-Sud (International Cooperation South South).
Project Website: www.refuge-ed.eu
Principal Investigator(s) (TCD): Dr Frédérique Vallières (TCD Lead), Prof Teresa Sordé Martí (PI)
Contact: Dr Sadhbh Byrne (byrnes83@tcd.ie)
Funding Agency: European Commission
Programme: H2020-SC6-MIGRATION-2020 (No. 101004717)
Funding Amount: €2,997,830
CONTEXT
Project Title: CONTEXT - The Collaborative Network for Training and Excellence in Psychotraumatology:
Summary: An international, interdisciplinary collaboration between nine European partner organisations CONTEXT is a doctoral training programme which takes place across the academic, non-governmental, voluntary, and public sectors. A total of 12 research fellows will conduct research with one of the following three Global Mental Health priority populations in Europe: (1) EU-based asylum seekers and refugees; (2) Emergency-service personnel and humanitarian first-responders; and; (3) Survivors and perpetrators of childhood- and gender-based violence. Each research project is designed to address current and emergent skill and professional deficiencies, essential for curbing the adverse social consequences of trauma-related psychological distress.
Partners: Ulster University; University of Southern Denmark; International Federation of the Red Cross, Red Crescent Psychosocial Reference Centre; Police Service of Northern Ireland; Dublin Rape Crisis Centre; Probation Board of Northern Ireland; Danish Children Centres; Spirasi
For more information: www.psychotraumanetwork.com
Principal Investigator: Dr Frédérique Vallières
Funding Agency: European Commission
Programme: H2020-MSCA-ITN-2016 (No. 722523)
Funding Amount: €3,316,000
Perform2Scale
Project Title:Perform2Scale
Summary: Perform2Scale uses a problem-based management strengthening intervention to improve workforce performance and health service delivery in three African countries: Malawi, Uganda, and Ghana. The goal of Perform2Scale is to develop and evaluate a sustainable approach to scaling up a district level management intervention in different and changing contexts.
Partner: Liverpool School of Tropical Medicine (Lead Coordinator); Royal Tropical Institute, Amsterdam; Swiss Tropical Institute; Makerere University, Uganda; University of Ghana; Reach Trust, Malawi.
Project Website: http://www.perform2scale.org
Principal Investigator (TCD): Dr Frédérique Vallières
Funding Agency: European Commission
Programme: H2020-SC1-2016-RTD
Funding Amount: €7,689,009
MRC
Project Title: Understanding and measuring pregnancy-related anxiety in low- and middle-income contexts: A pilot study in northern Ghana.
Summary: Prenatal anxiety has been associated with poor health outcomes of mothers and children, but much of the evidence is based on high-income nations using measures that have been developed for the use in Western populations. Hence, we need first to systematically review research on prenatal anxiety in order to get a clear overview of levels of pregnancy-related anxiety and relations with maternal and neonatal mortality. Then, we will apply a bottom-up approach, using focus group discussions to investigate the domains of pregnancy-related anxiety in Ghanaian women. This will inform the adaptation and validation of a measure of prenatal anxiety that is culturally relevant and adapted to the context in Ghana. The adapted measure will be pilot tested in a survey study of 575 pregnant women in northern Ghana.
Partners: Dr Hamideh Bayrampour (University of British Columbia), Ghana Medical Help
Principal Investigators: Drs Kristin Hadfield (TCD) and Gilbert Abiiro (University for Development Studies)
Funding Agency: UK Medical Research Council
Programme: Global Maternal and Neonatal Health 2019
Funding Amount: £89,808
FIERCE
Project Title: FIERCE - Evaluating the efficacy of a Jordanian shared book-reading intervention to improve early childhood education
Summary: Community-led, shared book-reading interventions can improve early childhood development and reduce inequity. One such program, We Love Reading (WLR) was implemented in Jordan in response to the Syrian refugee crisis and involved mothers reading stories to children. We will examine the potentially transformative nature of WLR, by (a) evaluating WLR qualitatively and quantitatively and (b) interviewing the people who developed and implemented WLR (WLR Ambassadors, women trained in WLR, children who too part) to create a toolkit for effectively developing and implementing non-formal education resources elsewhere. To address the first aim, we will conduct a grounded theory analysis of interviews with stakeholders (i.e. parents, children) and will conduct a quantitative randomized controlled trial with Syrian refugee women and children. This will allow us to understand how an education intervention may impact children's educational trajectories during war and displacement, and how we can effectively intervene in other humanitarian crisis contexts.
Partners: Prof. Amal A lKharouf (University of Jordan), Prof Sophie von Stumm (University of York), Taghyeer Foundation
For more information: https://www.thebritishacademy.ac.uk/projects/education-learning-in-crises-developing-implementing-transformational-intervention/
Principal Investigators: Drs Kristin Hadfield (TCD) and Isabelle Mareschal (Queen Mary University of London)
Funding Agency: British Academy
Programme: Education and Learning in Crises
Funding Amount: £359,490
TCD PhD Provost Award
Project Title: Improving the Psychological Treatment of Refugees and Asylum Seekers who have experienced torture and other forms of extreme trauma
Summary: The growing number of refugees is of particular concern to global mental health practitioners. Specifically, refugees are more likely to be trauma-exposed, and are at least 10 times more likely to experience posttraumatic stress disorder (PTSD) compared to the general population. The current project will (i) assess the cross-cultural utility of the International Trauma Questionnaire (ITQ), as a valid and reliable tool to measure PTSD and CPTSD among torture survivors, as per ICD-11 categorisations; (ii) determine whether a diagnosis of CPTSD differentially predicts patient outcomes over time, as assessed by a range of psychological outcome measures.; (iii) determine whether using patient-centred approaches, the most appropriate and acceptable psychological treatment paths for asylum seekers and refugees who meet the diagnostic criteria for PTSD or CPTSD.
Partners: Spirasi - The National Centre for the Rehabilitation of survivors of torture in Ireland.
Principal Investigator (TCD): Dr Frédérique Vallières (PI)
Contact: Aisling Hearns (hearnsai@tcd.ie)
Funding Agency: PhD Provost Awards (TCD)
Funding Amount: €95,000
FFPSS
Project Title: FFPSS - The effectiveness, mechanisms of change, and acceptability of Family Focused Psychosocial Support for at-risk adolescents in Lebanon
Summary: This mixed-method study aims to develop and evaluate a Family Systemic Intervention Module, named Sawa A2wa (Stronger Together), to use alongside UNICEF Lebanon's focused psychosocial support (FPSS) programme, to enhance current humanitarian programming and address a significant weakness of the current evidence base for at-risk adolescents and their families in conflict-affected contexts. Focused psychosocial support aims to promote wellbeing and resilience and to reduce mental ill-health in young people at risk of child protection violations, including gender-based violence, child marriage, and child labour. The immediate impact of the study is the focused support for 351 at-risk adolescents and their caregivers. Other impacts include the integration of the systemic family module into existing FPSS activities across Lebanon, and engagement with the National Mental Health Programme for longer term impact on psychosocial support provision.
Academic Partners: Dr FL Brown and Prof M Jordans (War Child Holland), Dr Maliki Ghoissany (Boston University), Dr T Betancourt (Boston College of Social Work), Prof A Carr (University College Dublin), Prof M Donnelly (Queen's University Belfast)
Technical and Implementing Partners: The Danish Refugee Council, Terre des Hommes Italia, War Child Holland, UNICEF Lebanon, the National Mental Health Program, the Global Health Institute and Community Advisory Boards
For more information: https://gtr.ukri.org/projects?ref=AH%2FT007419%2F1
Principal Investigator: Dr Tania Bosqui (TCD)
Funding Agency: Arts & Humanities Research Council (AHRC)/DFID
Programme: Development Grants
Funding Amount: £485,556
COVID-19 Psychological Survey
Project Title: COVID-19 Psychological Survey
Summary: The COVID-19 Psychological Survey is a multi-wave study running throughout the COVID-19 outbreak to better understand how people are responding, understanding, and coping with the pandemic. Data is being used to map changes in response to the evolving COVID-19 pandemic, people’s mental health, and views on COVID-19 vaccination. Three waves of data collection have taken place so far, the first of which took place two days after the initial lockdown.
Partners: Part of a six-country, international research consortium, the Irish arm of the survey is being conducted by the Trinity Centre for Global Health (Dr Frédérique Vallières), in collaboration with Maynooth University (Dr Philip Hyland), Ulster University (Professor Jamie Murphy, Professor Mark Shevlin), Edinburgh Napier University (Professor Thanos Karatzias), and University of Sheffield (Professor Richard Bentall).
Principal Investigator (TCD): Dr Philip Hyland & Dr Frédérique Vallières
Project Website: https://www.sheffield.ac.uk/psychology-consortium-covid19
Funding Agency:: Economic and Social Research Council (No. ES/V004379/1) ;with start-up funds from the University of Sheffield (Department of Psychology, the Sheffield Methods Institute and the Higher Education Innovation Fund via an Impact Acceleration grant administered by the University) and by the Faculty of Life and Health Sciences at Ulster University.
AIDS HIV
Dr Fiona Larkan and Dr Eilish McAuliffe are leading the Centre's research initiatives in the area of HIV/AIDS. Presently, we are developing initiatives which aim to address:
- The relationship between socio-structural-environmental context and reproductive behaviour among various disadvantaged population groups in sub-Saharan Africa, notably young women in rural Zimbabwe and adolescent slum inhabitants in Anglo-phone West Africa
- The role of adult heterosexual men in facilitating the spread of HIV has increased the need for more information to understand the dynamics between men's heterosexual behaviour and the spread of HIVAIDS in many populations all over the world. Research in this area has become more urgent given the increasing migration of young unmarried men from areas of high prevalence to areas of low prevalence.
The unprecedented economic boom of the "Celtic Tiger" has made Ireland, a country with low HIV prevalence, an important destination for migrant workers from Africa, Asia, Europe, the Middle East and South America. Since the majority of migrants are unaccompanied, it is important to investigate their patterns of sexual behaviour and the implications for the spread of HIV/AIDS and the health system in Ireland.
CAROLINE
Project Title: How Community Conversations influence behavior change communication for health: A realist evaluation in Marsabit, Kenya.
Summary: This is a 36-month Irish Research Council Marie Skłodowska-Curie Actions (MSCA) COFUND Postdoctoral Fellowship Programme entitled CAROLINE – ‘Collaborative Research Fellowships for a Responsive and Innovative Europe’. As part of CAROLINE, fellows will focus research on aspects of the Sustainable Development Goals (SDGs) and have inter-sectoral, international collaboration. This project will use realist evaluation methodology to understand how an NGO implemented intervention aimed at community systems strengthening and behaviour change works, for whom, and why, within Marsabit County, Kenya.
Partner: Concern Kenya, Concern Worldwide, World Health Organization
Principal Investigator(s): Dr Brynne Gilmore & Dr Frédérique Vallières
Funding Agency: Irish Research Council and European Commission
Funding Amount: €200,000
SPHEReS
Project Title: SPHEReS - Strengthening Post-graduate Health Education and Research in Sudan
Summary: Strengthening the management, performance, education and training of Human Resources for Health are all identified as priority areas in Sudan’s National Health Sector strategies (2012-2016). Aligned to the mission and strategic direction of the Sudan Medical Specialisation Board (SMSB), to improve the performance of the health system through standardised and monitored training, accredited training sites, qualified and committed trainers, and competent professional trainees, a new partnership was proposed between the SMSB and the Centre for Global Health, Trinity College Dublin.
Partner: Sudan Medical Specialization Board
Principal Investigator(s): Dr. Ayat Abu-Agla & Dr. Frédérique Vallières
Funding Agency: ESTHER-Ireland
Funding Amount: €8,000
Access to Infant and Maternal Health
This project is funded by World Vision, Irish Aid and DfID.
Aim
Assessing the use of community-based approaches to improve maternal and child health through addressing the most common preventable causes of infant and maternal morbidity and mortality.
Background
Growing enthusiasm around information communication technology for development (ICT4D) has sparked international interest and large investments in mobile phone projects across the globe. This technology has the potential to increase health service delivery; strengthen health information systems; improve data collection and monitoring; and provide support for health workers. The evidence demonstrating the impact of mobile phones as a human resource management tool for CHWs however, remains scarce.
The Trinity Centre for Global Health is partnering with the Ministry of Health and Sanitation Sierra Leone, World Vision Ireland and World Vision UK to improve maternal, newborn and child health in Bonthe District, Sierra Leone. Through grants from both Irish Aid and DFID, 33 CHWs will be trained in the delivery of the 7-11 timed and targeted counselling strategy. 7-11 is an evidence-based framework delivering 7 key health interventions for pregnant women and 11 key health interventions for children under 2.
The main objective of this study will be to carry out a piece of operational research to assess changes in health worker motivation over time, triggered by the introduction of a mobile phone application for 7-11 timed and targeted counselling as a specific human resource management tool. Motivation will be looked at in conjunction with performance indicators (i.e. referral rates, missed visits), supportive supervision, job satisfaction, and organisational commitment, all of which will serve as indicators of future attrition rates for the community health worker programme.
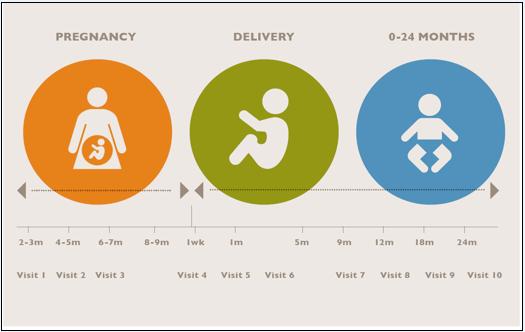
Fig. 1 TTC Visit Schedule
Evidence Aid
| Downloadable Materials |
|---|
| Identifying and Meeting the Need for Systematic Reviews in Disasters[239KB] |
People and organisations planning for and responding to natural disasters and other large scale emergencies need access to high quality, unbiased information on what works, doesn’t work and is unproven, if they are to make well-informed decisions that will help individuals and communities to recover. This information has to cover a wide variety of areas, including health, shelter, communication, construction, education, security and support for displaced people. It must be accessible, reliable and up to date. Evidence Aid will achieve this by working with those who require this information, the producers of the information, and others who can transfer knowledge and needs between the producers and the users.
Systematic reviews
Systematic reviews provide the vehicle by which evidence from research can be brought together in ways that minimise bias, avoid undue emphasis on single studies, and maximise the power of work that has already been done. They begin with a focused question and clear eligibility criteria; seek out and appraise the relevant studies; and compare, contrast and, where relevant and possible, combine their findings. They provide decision makers and others making choices with a summary of the available evidence, which can then be combined with other information, such as local values and resources, to take action. An up-to-date systematic review allows well-informed decisions to be taken more quickly and eases the evidence-gathering burden for people who need to take these decisions. The value of systematic reviews is recognised across many disciplines and the concept of drawing on the totality of evidence when making decisions is neither new nor outlandish when explained to researchers, policy makers and the public.
History of Evidence Aid
Evidence Aid was established by The Cochrane Collaboration, the world’s largest organisation dedicated to preparing and maintaining systematic reviews of the effects of healthcare interventions. The initial aim of Evidence Aid was to improve access to information for people and organisations facing health and healthcare challenges that arise in natural disasters and other large scale health emergencies and crises. It grew out of The Cochrane Collaboration’s response to the Indian Ocean tsunami in December 2004, when priorities were identified by people in the affected region and the Collaboration sought to provide relevant evidence.However, there were many gaps in the evidence base, and many problems with getting the information to the people who needed it. This was reinforced when the Collaboration responded to subsequent natural disasters such as the Wenchuan province earthquake in China in 2008, and the Haiti earthquake and Pakistan floods in 2010. It was also clear that although providing access to knowledge after the event can lead to benefits, it needs to be made available earlier as well, to the people and organisations preparing plans and procedures for disaster risk reduction and disaster response. It is also clear that evidence on health care is just one part of the myriad range of knowledge needs for natural disasters, and Evidence Aid is expanding, both in coverage and in partnerships, to provide a resource to meet those needs.
Evidence Aid - now
Evidence Aid has grown since 2004, with a steadily increasing collection of summaries of Cochrane reviews available free of charge on the internet and a limited, unfunded capability to respond to major natural disasters. For example, we provided a collection of resources to the World Health Organisation (WHO) and others within 24 hours of the devastating earthquake in Haiti in January 2010, providing information on interventions that are effective and on those that have been shown to be ineffective in areas such as fracture and wound management, mental health and infectious diseases.In August 2010, we worked with WHO and others on a special collection of Cochrane reviews to assist with the response to the widespread floods in Pakistan.The Cochrane Collaboration funded a formal evaluation of Evidence Aid in 2008/09, which highlighted the need for Evidence Aid to engage more closely with people and organisations involved in disaster risk reduction and response, and to improve awareness of, and accessibility to, its content.We are now implementing the findings of that evaluation.
Evidence Aid - next
In 2010, The Cochrane Collaboration set aside £25,000 to support part of the salary for a coordinator to work on Evidence Aid for an initial period of one year, to establish and strengthen contacts with key agencies in disaster relief. This funding was supplemented by £20,000 from Wiley-Blackwell, as a founding sponsor of Evidence Aid. Wiley-Blackwell have also agreed to provide in-kind support for the development a new website for Evidence Aid and to work with other publishers to facilitate the inclusion of relevant materials from other sources, which would also be free to users. Dr Bonnix Kayabu was appointed as the Evidence Aid coordinator in December 2010, within the Trinity Centre for Global Health in Trinity College Dublin, Ireland.
This has allowed Evidence Aid to enter a new phase and to begin to grow beyond health care. The expansion of Evidence Aid will require engagement with evidence providers and knowledge sources in new areas so as to make it easier for those planning for disasters and other large scale emergencies, and for those trying to cope with their aftermath, to make well informed decisions about priorities, needs and responses.
Evidence Aid – the future
If Evidence Aid is to meet the needs of decision makers, it must identify those needs, seek the necessary information and provide this information in a readily accessible form. It will do this through the compilation of a needs-driven collection of systematic reviews. Attached to these reviews will be short, targeted summaries, highlighting the relevance of the findings to the specific issues being faced and providing ‘headline’ conclusions in a format that will allow decision makers to make choices based on answers to questions about the effects of options available to them. The full text of the review will be available to those who wish to delve into the details and, for those who wish to go deeper by examining the studies upon which the review is based, we will seek to link all of the underlying research papers for the review. Our vision is that this whole collection of knowledge, from the summary, through the systematic review, and into the individual articles will be readily accessible in a timely manner, through a variety of media, including the internet, paper and mobile phone technology. This will require partnerships with researchers, journals and publishers. Where systematic reviews do not exist, we will identify ways to get them done. Where reviews exist but are out of date, we will identify ways to get them updated.
The next steps
Achieving this vision for Evidence Aid will require new partnerships, new funding and new ways to deliver the knowledge. It will require full engagement with the users of the resources, to make the resources fit for purpose, and to ensure that they take appropriate account of local needs and values. Evidence Aid seeks to provide the information that will help people make well-informed decisions, it does not seek to tell people what to do. The recent funding from The Cochrane Collaboration and Wiley-Blackwell will allow this work to begin, building on the foundations that have been laid over the last six years. But, more is needed.
Knowledge needs have to be mapped out to identify the areas of uncertainty that arise in the aftermath of natural disasters across many different areas. Decision nodes will be attached to these pathways, to highlight the points at which evidence from research could provide knowledge that will allow people to make better choices. Relevant evidence will be identified or produced, so that it can be attached to these nodes; and then monitored to ensure that it remains relevant, reliable and up to date. Based on the list of priorities created after the Indian Ocean tsunami, and initial discussions with others engaged in disaster risk reduction and response, several hundred systematic reviews will be needed in health care and beyond. At this time, it seems likely that 200 systematic reviews in health care and 100 systematic reviews in other areas would cover the highest priorities. Approximately half of these healthcare reviews are already completed, but several need to be updated. Evidence Aid needs to begin to map these known reviews and those that are identified outside of the health care, to the priorities.
The identification of gaps will also arise during the development of the pathways and decision nodes that will be key to providing relevant knowledge to people making choices about disaster planning and response. This will be achieved by a thorough assessment of information that has already been gathered following recent natural disasters, and during other situations such as the mass displacement of populations due to famine or war. This will be supplemented by new evaluations, so that these can focus specifically on those aspects of decision making that Evidence Aid is most likely to be able to help with.
The expansion and strengthening of Evidence Aid will help those responsible for making decisions relevant to natural disasters to choose effective strategies and avoid those that are ineffective. It will bring benefits in the aftermath of disasters, as well as helping people making decisions in resource poor settings more generally. It will save lives, reduce morbidity and enable communities to recover quicker and more efficiently.
References
Tharyan P, Clarke M, Green S. How the Cochrane Collaboration is responding to the Asian Tsunami. PLoS Medicine2005;2(6):e169.
Clarke M. Evidence Aid - from the Asian tsunami to the Wenchuan earthquake. Journal of Evidence Based Medicine2008;1:9-11.
Turner TJ, Barnes H, Reid J, Garrubba M. Evidence for perinatal and child health care guidelines in crisis settings: can Cochrane help? BMC Public Health 2010;10:170.
http://www.thecochranelibrary.com/
http://www.thecochranelibrary.com/
Turner T, Green S, Harris C. Supporting evidence-based health care in crises. What information do humanitarian organizations need? Disaster Medicine and Public Health Preparedness 2010, published online prior to print (October 26 2010).
For further information on this research programme please contact Prof. Mike Clarke, Principal Investigator
For more information please visit:
Participation in Evidence Aid Survey
Needs assessment of aid agencies and funding organizations on the use of systematic reviews in disaster settings
We are inviting people working in the humanitarian sector and other related areas to take part in a survey as part of the Evidence Aid project. This examine the use of systematic reviews by decision-makers involved in, planning for and responding to natural disasters and other humanitarian crises.
Evidence Aid was initiated by The Cochrane Collaboration and has grown to include new partners. This survey is being carried out in collaboration with the Trinity Centre for Global Health, Trinity College Dublin, Ireland and is being supervised by Professor Mike Clarke, from the Centre for Public Health in Queen’s University Belfast, Northern Ireland, (former Director of the UK Cochrane Centre). This survey has been made possible by funding to Evidence Aid from The Cochrane Collaboration, Wiley-Blackwell and the European Union funded TENALEA project", to the cover letter and the survey.
Evidence Aid uses knowledge from Cochrane reviews and other systematic reviews to provide reliable, up-to-date evidence on interventions that might be considered in the context of natural disasters and other major emergencies. We are seeking to highlight which interventions work, which don’t work, which need more research, and which, no matter how well meaning, might be harmful; and to improve access to this information.
Systematic reviews aim to identify, appraise and summarize the findings of relevant research on a given topic, to make the available evidence more accessible to people making decisions and setting policy. They compare and contrast the findings of individual studies, and, when appropriate, combine the results to provide a more reliable and precise estimate of the effect of an intervention, or the association between variables, than is possible with a single study. They can be done in any area of research, but by far the largest proportion currently available are related to health. Cochrane reviews are produced by The Cochrane Collaboration and focus on the effects of healthcare interventions. The Cochrane Collaboration is the world's largest organization dedicated to the production of systematic reviews, with more than 4500 reviews published to date, through the work of 25,000 volunteers in over 100 countries.
Your participation in this survey will help us to draw up a list of priority topics for evidence relevant to needs following natural disasters and other humanitarian emergencies. The priority topics will then be described to allow the identification of potentially relevant systematic reviews and the underlying research. This will supplement the list of topics drawn up following the 2004 Asian-Pacific tsunami, the floods in Pakistan, the earthquake in Haiti and the current Japanese disaster.
This study will contribute to good practice and will enable humanitarian intervention planners and beneficiaries alike to have access to information based on evidence before, during and after natural disasters, and other complex emergencies throughout the world.
Participation in the study was voluntary and entirely confidential – personal details of respondents will not be disclosed. Participants will be able to choose the language they wish to respond in (English, French, Spanish or Arabic).
 Dr. Bonnix Kayabu
Dr. Bonnix Kayabu
Coordinator, Evidence Aid
E-mail: kayabumb@tcd.ie)
Landline: +353 1 896 4395
STEM (Support, Train and Empower Managers)
This project is funded by the European Union and Irish Aid
http://ec.europa.eu/europeaid/
Background
![]()
The attainment of the Millennium Development goals (MDG) by the target date of 2015 is unlikely given the depleted capacity of many health systems to respond to their populations’ health needs (Joint Learning Initiative, 2004). It has therefore been suggested that countries need to move away from the expensive production of clinically oriented health professionals to focus instead on the more pragmatic production of health workers appropriate to their burden of disease, availability of resources and minimum standards of care (Huddart & Picazo, 2003). Indeed this strategy has already been adopted by several countries who are increasingly relying on mid-level cadres, such as medical assistants, clinical officers and enrolled nurses to provide health care (Buchan & Dal Poz, 2003). These cadres have shorter lengths of training than doctors or registered nurses. A recent review of mid-level health workers (WHO, 2009) suggests that more than 100 different categories of mid-level workers have been used to provide health care, particularly to underserved communities, and that this use has been widening in both high- and low-income countries. While the review notes that utilisation, skills, length of training and management practices vary quite substantially across cadres and countries, it highlights the success of Asian countries in developing a large number of local mid-level worker categories, from birth attendants to health assistants, who are not modelled on traditional health professions, but respond to specific country needs.
Mid-level cadres are well established within the public health systems of Mozambique and Tanzania. Recent studies provide strong evidence for the clinical efficacy (Chilopora et al., 2007; Pereira et al.,2007; McCord et al, 2009) and economic value (Kruk, et al, 2007) of these cadres, particularly in the provision of emergency obstetric care. Given such positive indicators it is important to recruit, retain and support these cadres to build the capacity of health systems in low-income countries. Educational qualifications that are less marketable internationally make it less likely that these staff will migrate. However, the belief that these cadres are not internationally marketable has given rise to some complacency in the management and motivation of such workers (McAuliffe et al, in press). Many countries introduced them as a short-term measure with the anticipation that once the country built up its stock of health workers they would no longer be needed. Because of this there has been little investment in developing their skills or their career pathways, which undoubtedly impacts on their motivation and relationships with other healthcare professionals (McAuliffe et al. 2009a).
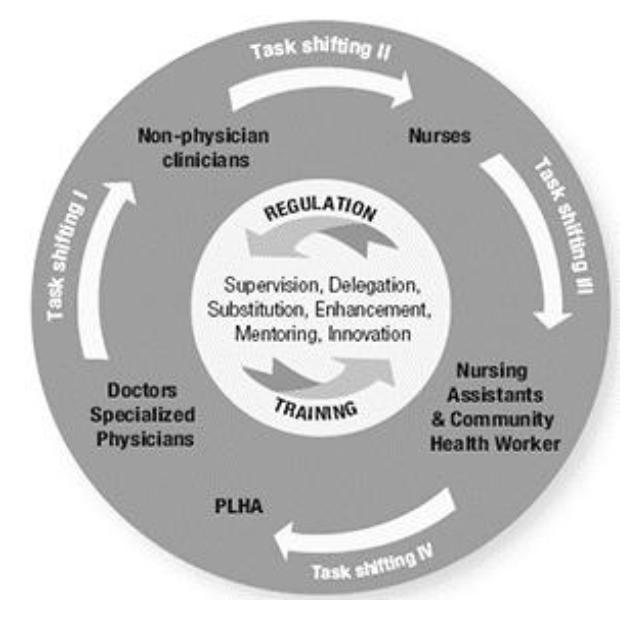
Fig. 1 The WHO concept of Task Shifting.
However, as the costs associated with training and retaining internationally recognised health professionals become prohibitive, many African countries are turning their attention towards non-physician clinicians and other mid-level cadres. There is cumulative and strong evidence for the effectiveness of task shifting to alternative - or so-called ‘mid or low-level’ – cadres (McPake and Mensah, 2008; McCord et al, 2009). Figure 1 illustrates WHO’s working concept of task shifting, where specific tasks can be reallocated from more to less specialised personnel. At the core of this model are the important tasks of training and regulating, activities that are underpinned by mentoring, support and supervision.
Objective of the project
The overall objective of the proposed project, STEM - Support, train and empower managers, is to strengthen the human resource management (HRM) function at district and health facility level, by increasing the capacity of managers to support and supervise their staff. This will be achieved by the introduction of a systematic and structured approach to support and supervision of health workers in Tanzania and Mozambique (many of whom fall into this category of mid-level cadres or non-physician clinicians).
Research Partners
Ifakara Health Institute, Tanzania |
|
Eduardo Mondlane University, Mozambique |
For further information on this research project please contact Dr Ogenna Uduma, STEM Project Manager.
Project Team Meetings at the Trinity Centre for Global Health, TCD (26th January - 1st February 2012)

Back row, from left: Dr Tavares Madede, EMU; Ms Susan Bradley, CGH; Mr Fred Lwilla, IHI; Dr Henry Mollel, IHI; Ms Sara Melo, CGH; Mr Jonas Chambule, IA, Mozambique; Sitting in front, from left: Dr Mohsin Sidat, EMU; Dr Eilish McAuliffe, CGH; Dr Masanja Honorati, IHI.
Project Team Meetings in Arusha, Tanzania (9th - 14th December 2013)

STEM Team with the district representatives.
ADD-UP (Aid salary discrepancies and development workers' performance)
Funded by ESRC/DiFD
This research project is jointly co-ordinated by Professor Stuart Carr, Poverty Research Group, Massey University, New Zealand and Professor Mac MacLachlan, Trinity Centre for Global Health, Trinity College Dublin, Ireland. According to the Paris Declaration best practice in aid work means pay should be aligned and harmonised across worker groups (World Bank, 2005). Although pay may not be a primary motive for development workers, discrepancies in pay nonetheless have the potential to influence perceptions of organisational justice, which can in turn affect work performance. Moreover, because injustice is a motivation for much aid itself, perceptions of unfairness in aid work may have an inherent salience and undermine its necessary constituents, especially cooperation and capacity building. This project explores the effects of aid salary discrepancies in the health, education and business sectors of six countries: the landlocked economies of Malawi and Zambia; the transition economies of India and China; and the island economies of the Solomon Islands and Papua New Guinea. Bringing together an international team of psychologists and sociologists from 10 different countries this project focuses on the human dynamics of aid salary discrepancies and their significance for capacity building in low-income countries.
Dual Salaries and Project ADDUP: Are Development Discrepancies Undermining Performance?
A fair day’s work for a fair day’s pay.
Carlyle’s adage reminds us that decent remuneration is integral to the International Labour Organisation’s “Decent Work Agenda.” Yet in many lower-income settings, there is a glaring institutional inequity: Dual salaries. Compared to local colleagues performing the same or similar jobs, expatriate workers are usually paid much more.
This double standard is not simply about gaps in skills or experience. Many lower-income countries have invested well in local education and training since Independence. International salaries are higher mainly because expatriates originate from higher-income economies, and labour markets. The resultant gaps contravene Paris and Accra declarations on aid effectiveness, which instead promote harmonisation and alignment. They are also, arguably, discriminatory.
An Elephant in the Development Parlour.
Contravention of initiatives to improve the effectiveness of aid may partly explain why the topic remains taboo - and under-researched. Project ADDUP acknowledges the elephant in the parlour, and breaks the silence. A multi-disciplinary study reflects the voices of over 1300 professional workers and community representatives from 200 aid, government, educational and business organisations in land-locked (Malaŵi, Uganda), Oceanic (Solomon Islands, Papua New Guinea) and emerging economies (India, China).
ADDUP systematically explores the human dynamics of dual salaries, by: (a) documenting the extent of salary discrepancies; (b) exploring their consequences for work performance; and (c) determining the potential for salary alignment and harmonization to boost cooperative work performance, build capacity and more effectively reduce poverty.
The Project
We began by asking workers to provide “critical incidents,” or work stories, about dual salaries and their daily impacts on capacity development. Based on these incidents, we designed a radically new survey instrument. Participants answered questions about their remuneration levels and standard of living, remuneration-comparison, -justice, -motivation, job satisfaction, work engagement, turnover and thoughts about global mobility. We ran control measures of cultural values, culture shock, and a range of demographic variables, e.g., gender, highest qualification and years’ experience. At the conclusion of the survey phase we took the data back to the communities from which they were lent. There, subject-matter-experts and key stakeholders interpreted our initial analyses of the data for their practical and moral value.
Local Relevance
The main findings are that: (a) excluding a negligible number of local respondents on international remuneration and expatriates on local pay, ratios in purchasing power between international and local pay average 4:1, leaving most local workers in economic need. The greatest disparity occurred in Island Nations (approaching 9:1); the least in emerging economies (approximately 2:1); with landlocked nation’s in-between (3:1).
Multi-level modeling highlighted a resultant (b) sense of injustice among the locally-remunerated workers, which was the major predictor of work motivation/de-motivation. This together with job satisfaction and work engagement predicted turnover and international mobility intentions - brain drain.
According to subject-matter experts who interpreted the findings via in-country workshops, these data indicate that (c) closer harmonization and alignment of dual salaries would reduce poverty directly among workers, boost cooperative work performance, build capacity, and help reduce poverty. A range of technical options for closing the gap, and enhancing equity, were suggested.
Global Dissemination
These findings are set to appear in the peer-reviewed flagship journal of the International Union of Psychological Science, the International Journal of Psychology (2010). The findings have reached a range of workshops and keynote addresses at development-related conferences, such as the Annual Global Development Network meeting (2008) and at the “Psychology Serving Humanity” conference in Cape Town, by the international Union of Psychological Science (for 2012).
The findings from addup also inspired a ground-breaking new book, The aid triangle: recognizing the human dynamics of dominance, justice and identity (May 2010, MacLachlan, Carr & McAuliffe, Zed Books, London and New York).
Impact
Project ADDDUP has been instrumental in the setting-up of a first Global Task Force for Humanitarian Work Psychology (http://www.humworkpsych.org). This is an international network of researchers and practitioners from lower-, middle- and higher-income countries, whose goal is to promote and build capacity by applying humanitarian principles in work settings through multilateral bodies such as the United Nations and the International Labor Organisation, as well as with policy think-tanks like the Organisation for Economic Cooperation and Development (OECD).
The Task Force has just submitted our first full submission to the United Nations through its call for fresh perspectives on Keeping the Promise (UN, 2010). We argue that organisations have become a forgotten entity in the development equation, falling between the twin stools of macro-economic policy and micro-psychological analysis.
Our data from Project ADDUP clearly suggest that organisations can be points of intervention to enable a fair day’s work for a fair day’s pay.
Acknowledgment
Project ADDUP was funded through the ESRC and DFID Joint Scheme for Research on International Development (Poverty reduction).
One-minute Elevator Test
The project identifies a range of barriers to basic capability and capacity development, taking place in workplaces across a range of sectors, due to dual salary policies: (1) remuneration leaves locally-salaried workers, chiefly local people, below the poverty line, defined as not meeting everyday needs; (2) technical cooperation is impeded by the sense of injustice and comparative disadvantage that permeate dual salary systems; (3) organisational climate is a moderator of the linkages in (2), implying that organisations can become points of intervention to render pay and benefits more fair, and thereby improve human services, productivity, and poverty reduction itself. The UN’s latest publication Keeping the Promise of the Millennium Development Goals calls for greater attention to organisations, and the human factors in them.
ChRAIC (Irish African Partnership for Health Research Capacity Strengthening)
This five year Ireland Africa Partnership, started in 2008, focuses on pro-poor research to address the Health MDGs: reducing child mortality; improving maternal health and controlling HIV/AIDS, malaria and other infectious diseases.
The goal of the Partnership, in support of the Government of Ireland’s development goals, was:
- to build research capacity in Ireland and Africa and
- to conduct research that strengthens health systems in Africa to serve the poor more effectively
The main Programme themes were:
- Governance: research that contributes to strengthening the capacity of government institutions and the involvement of civil society and other stakeholders in providing services that meet the health needs of the poor.
- Human resources for health: research to identify strategies for ensuring that health workers are available, able and motivated to deliver health services, especially to those who are poor or marginalised.
- Access and Equity: research that contributes to understanding and overcoming barriers that the poor and other disadvantaged groups experience in seeking to access health services.
Partners included: Trinity College Dublin, The Royal College of Surgeons in Ireland, The National University of Ireland Galway, the Malaria Consortium, and Institutes in Lesotho, Malawi, Mozambique, Sierra Leone, Sudan and Uganda.
Year 1 activities involved research mapping through reviewing country literature on key themes, awarding PhD scholarships and training PhD candidates, and building local research capacity.
For further information on this research project please contact Dr Steve Thomas, TCD Principal Investigator.
A-PODD (African Policy on Disability & Development)
Downloadable Materials |
|---|
In_Brief_SIERRA_LEONE [728KB] |
In_Brief_UGANDA [468KB] |
In_Brief_ETHIOPIA [647KB] |
In_Brief_MALAWI [981KB] |
A-PODD (African Policy on Disability and Development) was a three-year qualitative research project, funded by a €500,000 research grant from the Health Research Board/Irish Aid. A-PODD was led by Prof Malcolm MacLachlan, Trinity Centre for Global Health and School of Psychology, Trinity College Dublin. The Trinity Centre for Global Health’s primary coordinating partners on this project were Ms. Gubela Mji at the Centre for Rehabilitation Studies, Stellenbosch University and Mr. Kudakwashe Dube at The Secretariat of the African Decade for Persons with Disabilities, South Africa.
This research investigated the need for disability to be included on the agenda of national and international development initiatives. It aimed to document and analyse the factors that contribute to realising the rights of disabled people, promote their health and well-being and release their economic potential, with government strategies aimed at poverty alleviation. It focused on how research evidence can be utilised to inform the policy environment (such as PRSPs and SWAps), and development institutions (such as the IMF, World Bank and WHO). The research also focused on less formal local, community and grass-roots decision-making and inclusion efforts.
A-PODD undertook four country-case studies:
Sierra Leone, a country emerging from conflict that resulted in many people being disabled;
Malawi and Uganda, the only two African countries that have Ministries for people with disabilities;
Ethiopia, the second most populous country in Africa, with significant geographical barriers and a highly dispersed population, presenting significant challenges to the inclusion of people with disability.
The disabled people in Africa constitute a valuable resource for economic growth, if this economic potential can be realised. Key to this is their access to healthcare, education and housing. In addition to promoting innovative redistribute policies, the project sought to involve disabled people as part of the economic solution to achieving the Millennium Development Goals (MDGs), particularly poverty reduction.
Recently, the approach to disability has changed dramatically from a charitable, paternalistic and biomedically-based ‘caring-for’ approach. This approach recognises the human rights of disabled people and their need for advocacy and empowerment, in order to fully participate and be included in society.
A comparative analysis informed the disability policy within the region. Factors which restrict or facilitate these policies were identified along implementation pathways, as were local means and mechanisms of addressing them. Country reports were discussed at the concluding workshop to which governments, civil society, donors, researchers and others were invited. A code of best practice wes drawn up for Moving Evidence to Action on African Disability Policy.
The A-PODD (African Policy for Disability and Development) website has now been established (www.a-podd.org). There is an interactive function on the A-PODD website and we would be pleased if you would like to 'post' any comments or suggestions. The public may register on this website, so we will have a database of users that we can communicate with also.
Post-Doctoral Research Fellows (based in Stellenbosh University):
Dr. Margaret Wazakili (mwazakili@sun.ac.za)
Dr. Tsitsi Chataika (tchataika@sun.ac.za)
Project Co-Ordinator: (based in Trinity College Dublin):
Mrs. Marcella Maughan
For further information on this research project please contact Prof. Mac MacLachlan
EquitAble: Enabling universal and equitable access to healthcare for vulnerable people in resource poor settings in Africa
The consortium was led by Professor Mac MacLachlan (Trinity Centre for Global Health & School of Psychology), with Trinity Co- Investigators, Dr. Hasheem Mannan (National Institute for Intellectual Disability & School of Social Work & Social Policy) and Eilish Mc Auliffe, (Trinity Centre for Global Health & School of Medicine).
The consortium partners were:
- Afhad University for Women (Sudan)
- University of Malawi Centre for Social Research (Malawi)
- Human Sciences Research Council (South Africa)
- Secretariat of the African Decade for Persons with Disabilities (South Africa)
- The Foundation for Scientific and Industrial Research at the Norwegian Institute of Technology (SINTEF) (Norway)
- University of Stellenbosch Department of Psychology and the Centre for Rehabilitation Studies (South Africa)
- University of Namibia Multidisciplinary Research and Consultancy Centre (Namibia).
This research programme recognized that health services cannot hope to be equitable unless they are equally accessible to all. The project contributed to achieving the Millenium Development Goals (MDGs) by addressing the health service needs of some of the most disadvantaged people in Africa. Conceptualizing disability along a continuum of activity limitation the programme explored the interplay between disability and other factors that marginalize and exclude people from mainstream services and society. EquitAble used policy analysis along with qualitative and quantitative empirical research methods to contribute to a rigorous evidence-base that aims to bridge the know-how gap for national, regional, and international health policies and practice.
For further information on this research project please contact Prof. Mac MacLachlan
Project Website: http://www.equitableproject.org/
Downloadable Materials |
|---|
The EquiFrame Manual [2,953KB] |
| EquiFrame_write-up_in_The_Parliament [346KB] |
The EquiFrame Manual 2014_French version [1,766KB] |
HSSE:
Health System Strengthening for Equity:
The Power and Potential of Mid-level Providers
Funded by Irish Aid and the Ministry of Foreign Affairs, Denmark.
The human resources for health crisis in Africa demands innovative and locally appropriate solutions that increase access to quality health care at a price affordable to governments. One such solution is the development and deployment of mid-level providers as seen in many countries throughout Africa over the past four decades. These mid-level providers typically perform critical functions conventionally associated with more highly trained and highly mobile health providers and, compared to doctors, are more likely to be present at district level health facilities especially in rural areas.
Yet, despite apparent broad use of mid-level providers in Africa, these health workers are virtually invisible in policy documents and government strategic plans; there are few efforts to expand their training; and little is known about their current use and practice or even about the factors at individual, organisational, and environmental levels that enable or block their performance. To address this need, a consortium of four research, advocacy and policy focused organizations have formed a strategic partnership to implement the proposed project, Health System Strengthening for Equity: The Power and Potential of Mid-level Providers (HSSE). This is a four year, multi-country project that builds on the growing policy momentum and global dialogue to address the human resource crisis and the need to support functioning, responsive health systems. The four partner organizations are Trinity College Dublin Trinity Centre for Global Health (CGH), Columbia University's Mailman School of Public Health Averting Maternal Mortality and Disability Program (AMDD), Realizing Rights: the Ethical Globalization Initiative (RR:EGI), and the Africa-based Regional Prevention of Maternal Mortality network (RPMM).
HSSE Project Goal and Objectives
The goal of the Health System Strengthening for Equity project was to support health system strengthening for equity in Africa by building an evidence base on the role of mid-level providers in maternal and neonatal health and promoting greater political leadership and critical policy action on this issue. The strategy that drives this Health Systems Strengthening for Equity (HSSE) project had multiple elements:
- a) a unique and strategic collaborative partnership among research, policy and advocacy organizations, and among northern and southern institutions;
- b) an approach to collaborative research that builds and supports capacity in countries and that respects the principle of country ownership of its data;
- c) an approach to collaborative advocacy that builds capacity of both southern and northern institutions to use evidence for policy and to link global and national processes and debates in order to generate more realistic and sustainable solutions; and
- d) a commitment to supporting (and not undermining) ongoing policymaking processes and to ensuring the development of policy-relevant evidence and analysis.
The HSSE project focused on the delivery of emergency obstetric and newborn health care (EmONC) by mid-level health workers as a key entry point to assessing the use and effectiveness of mid-level providers more broadly. A multi-country approach enabled in-country analyses and cross-country comparisons. The main focus countries were Malawi, Mozambique and Tanzania as each country has well established cadres of mid-level providers delivering the bulk of emergency obstetric care (including caesarean sections).
Project Website: http://www.midlevelproviders.org/
LEARN PROJECT
The LEARN Project focused on addressing the challenges of organisational learning in international aid organisations. The project was funded by the Irish Research Council for Humanities and Social Sciences and had two corporate partners: Irish Aid and Concern. The Learn Team comprised four academic supervisors and four PhD students. We were interested in developing understanding and practical action for organisational learning. This involved researching the role of organisational sub-cultures (Lorraine Mancey), working relationships (Sarah Barry), advocacy and action research in relation to strengthening organisational learning systems. The LEARN Project was led by Prof. Mac MacLachlan (Principal Investigator).
Realist Researcher Group
The use of realist methodologies in Ireland is growing. This methodology can be both rewarding and challenging. The Trinity Centre for Global Health in Trinity College Dublin has established a working group for researchers currently using realist methods to provide peer support for this process. The Realist Researcher (Support) Group aims to provide a platform for realist researchers to share experiences and trouble-shoot the methodology with others involved in the field. Meetings will be held in Dublin, and the group is open to all individuals currently engaged in realist research both in academic and practice settings. Within the Trinity Centre for Global Health, we have partnered with World Health Organization (WHO) and World Vision Ireland using realist methodologies for reviewing evidence, programme evaluation and making recommendations. We have completed two commissioned, large-scale realist syntheses and have several other realist project underway as part of PhD research. For more information, or if you wish to join the group please email Jessica Power at odowdje@tcd.ie or Brynne Gilmore gilmorb@tcd.ie.
Community health Committees in Tanzania and Uganda.
Abstract: Strengthening community actions to improve participation in health is an essential part of health promotion and health systems strengthening. To this end, community health committees (CHC) are frequently utilised in low-income countries (LICs) to achieve a specific goal and build community capacity. Though some evidence is available on CHC’s contribution to health outcomes, currently unknown is how, and to what degree, such committees are most effective in building community capacity for improved health. This research therefore sought to explore how CHCs work to build community capacity by conducting a realist evaluation across multiple case studies in Tanzania and Uganda. Preliminary findings have been reported across several dissemination channels (see Publications below).
Contact: Brynne Gilmore
When Scaling Up How are Health Interventions Modified to Fit Local Settings: A Realist Synthesis.
Abstract: Health interventions are scaled up across diverse settings with differing needs and resources. In practice, modifications are often made to address this diversity however the processes used to make these decisions have not been fully researched.
This research is using a realist synthesis methodology to explore what processes were used across case examples of scale up to make decisions on modifications to the content of the intervention, context or delivery strategy. By using realist methodologies the research aims to discover under what circumstances these processes were used and what mechanisms and outcomes took place. This research has two phases with the first examining secondary data of published examples of scale up to develop and refine theories on these processes. The second phase will complete stakeholder consultations with health implementers to further refine and test these theories.
Contact: Jessica Power odowdje@tcd.ie
Research For Health in Humanitarian Crises (R2HC) seed funding: In collaboration with Liverpool School of Tropical Medicine (LSTM), University College Dublin (UCD) and International Medical Corps (IMC) in Turkey, Iraq and Lebanon, this work sought to understand the motivation and performance of community health workers (CHWs) within conflict settings. The CGH was awarded seed funding from the R2HC programme co-funded by DFID and the Wellcome Trust to develop an initial theory using realist evaluation and to propose a three-country realist evaluation for theory refinement.
Contact: Brynne Gilmore
WHO Commissioned Research: Guideline Recommendations for the Work Force for Community Based Rehabilitation in Less Resourced Settings: A Realist Synthesis.
This research sought to identify best practices for human resources for health-related rehabilitation within the overall context of health systems strengthening. It has a particular focus on the integration and decentralization of the rehabilitation workforce within the health systems of less resourced settings.
Contact: Brynne Gilmore
WHO Commissioned Research: Guideline Recommendations for Leadership and Governance for Health-Related Rehabilitation in Less Resourced Settings: A Realist Synthesis. This research aimed to identify best practices for leadership and governance (with a particular focus on policies) of health-related rehabilitation within the overall context of health systems strengthening. Our approach to establishing good policy practices has been to undertake a systematic literature review, a realist interpretation of the literature and a Delphi sampling of expert opinion; and to synthesize these to answer questions posed in the commissioning of this research.
Contact: Joanne McVeigh
Realist Researcher Group Publications and Presentations
Deimling Johns, L., MacLachlan, M., Power, J. 'Core skills associated with mental health intervention in community-based rehabilitation: A Realist Review'. 2nd International Conference on Realist Evaluation and Synthesis: Advancing Principles. Liverpool, UK. 2nd-6th October 2016.
Gilmore, B., McAuliffe, E. Larkan, F, Conteh, M., Dunne, N., GMollel, H. 2016, Tumwesigye, N.M., Vallières, F. How do community health committees build capacity for maternal and child health?: A realist evaluation protocol. BMJ Open 6(11), p.e011885.
Gilmore, B., Adams, B.J., Bartoloni, A., Alhaydar, B., McAuliffe, E., Raven, J., Taegtmeyer, M. & Vallieres, F. (in-press). Improving the performance of community health workers in humanitarian emergencies: A realist evaluation protocol for the PIECES programme. BMJ Open 6(8), p.e011753.
Gilmore, B., MacLachlan M., McVeigh J. Methodological challenges in using Realist Synthesis for Global Health Promotion. Presentation to the Realist Working Group at Third Global Symposium on Health Systems Research, October 1 2014, Cape Town, South Africa
Gilmore, B., MacLachlan, M., McClean, C., Carr, S., Duttine, A., Mannan, H., McVeigh, J., McAuliffe, E., Mji, G., Eide, AH., Hem, KG. & Gupta, N. 2014. ‘Realist Review: Recommendations for the Health Workforce for CBR’. Oral presentation at the International Association for Critical Realism, 17th Annual Conference, London, UK. 19 July 2014
Gilmore, B., Tumwesigye, N.M., Mollel, H., Conteh, M., Dunne, N., McAuliffe, E., Larkan, F. & Vallières, F. 2016 (oral ) How do community health committees build capacity for maternal and child health?: A realist evaluation in Uganda and Tanzania. Fourth Global Symposium on Health Systems Research: Resilient and Responsive Health Systems for a Changing World, Health Systems Global, Vancouver Canada, November 14-18.
McVeigh, J., MacLachlan, M., Gilmore, B., McClean, C., Eide, A. H., Mannan, H., Geiser, P., Duttine, A., Mji, G., McAuliffe, E., Sprunt, B., Amin, M., and Normand C. Promoting good policy related leadership and governance of health related rehabilitation: a realist synthesis. Globalization and Health 12(1), p.49.
McVeigh, J., Gilmore, B., MacLachlan, M., McClean, C., Carr, S., Duttine, A., Mannan, H., McAuliffe, E., Mji, G., Eide, AH., Hem, KG. & Gupta, N. 2014. ‘Realist Synthesis: Recommendations for CBR’. Oral presentation at the 1st International Conference on Realist Approaches to Evaluation and Synthesis: Successes, Challenges, and the Road Head. Liverpool, UK. 27-30 October, 2014
Muhumuza, J., Gilmore, B., Conteh, M., Dunne, N., Larkan, F., McAuliffe, E., Vallières, F. & Tumwesigye, N.M. 2016 (oral) Community Committees for Capacity Building: Lessons Learned from a Study in North Rukiga, Uganda. Fourth Global Symposium on Health Systems Research: Resilient and Responsive Health Systems for a Changing World, Health Systems Global, Vancouver Canada, November 14-18.
Power, J., Larkan, F., McAuliffe, E., Mannan, H. Scaling up Healthcare Interventions
The Need to Contextualise for Local Settings. Poster Presentation. 2nd Clinical Trial Methodology Symposium. Cork. 25th and 26th October 2016.
Power, J (O’Dowd, J.). The Role of Context in Delivering Complex Interventions. Taking a Realist Approach. Conference Presentation. 1st Clinical Trial Methodology Symposium. Dublin. 24th Sept 2015.
Wall, PJ. A Critical Realist Perspective on Mobile Health (mHealth) – A Case Study in Sierra Leone. Oral presentation at the International Association for Critical Realism, 17th Annual Conference, London, UK. 19 July 2014
MaxHR
Funded by the Advisory Board of Irish Aid.

This research was exploring the critical factors influencing human resource capacity to deliver equitable effective health care efficiently at the district level. The identification of constraints to HR planning and management at the district level as well as the key factors influencing staff retention and attrition contributed to the development of more effective human resource strategies that ultimately strengthen health systems at the district level. The research identified the critical factors influencing human resource capacity and performance at the district level. The research was focused on the District Health System (DHS) as the vehicle for the delivery of primary health care. As the research was concerned with motivational factors amongst conventional health workers and new cadres of health workers, the research population included district health managers, doctors and nurses (as the predominant conventional health workers) and new cadres of health workers (which include medical assistants, extension and community workers) working at DHS level.
Preparatory work was undertaken with Ministry of Health and district level personnel in Malawi to actively engage key stakeholders in the design of the research, in the interpretation of the findings and in the formulation of practical recommendations to improve human resource performance at the district level. This was in keeping with the action research methodology adopted in this research. A key contribution of the research process was its potential to build institutional research capacity to work in partnership with the health services towards finding practical solutions to difficult problems. This approach increased the likelihood of service improvements resulting from the research because of the shared ownership of the problem and the greater understanding generated through an active, ongoing involvement with the principal researchers. It also had greater potential (than traditional research approaches) to bridge the research to policy gap because ongoing dialogue with policy makers is inherent to the process. The work was focused on Malawi and Lesotho.
Collaborating Partners

- Department of Community Health, College of Medicine, University of Malawi
- Ministry of Health and Social Welfare, Lesotho
- Faculty of Health Sciences, National University of Lesotho
- Irish Aid Lesotho
- Centre for Health Informatics, The University of Dublin, Trinity College
- Department of Health Promotion, National University of Ireland, Galway
- Health Policy Unit, London School of Hygiene and Tropical Medicine
The Research Team
| Eilish McAuliffe | Trinity Centre for Global Health, TCD |
| Dr. Ogenna Manafa | Trinity Centre for Global Health, TCD |
| Prof. Malcolm MacLachlan | Trinity Centre for Global Health and School of Psychology, TCD |
| Prof. Charles Normand | Trinity Centre for Global Health and Health Policy and Management, TCD |
| Prof. Jane Grimson | Centre for Health Informatics, TCD |
| Prof. Cameron Bowie | Department of Community Health, College of Medicine, University of Malawi |
| Dr. Diarmuid O'Donovan | Department of Health Promotion, NUI Galway |
| Prof. Ruari Brugha | Department of International Health, Royal College of Surgeons in Ireland |
| Prof. Barbara McPake | Departament of International Health, Queen Margaret College, Edinburgh |
The MaxHR Project was led by Prof. Eilish McAuliffe, Principal Investigator.
The Motivation Project
There is a growing need to strengthen health systems in poor countries to help meet the Millennium Development Goals (MDGs). The challenge is made more difficult by the demands of the AIDS crisis, migration of skilled professionals to high income countries and low morale and motivation of remaining staff. These have combined to generate a rapid worsening of availability and quality of care. Improving the retention of health workers in developing countries is critical for health system performance. Consequently, this project focused on improving understanding of how best to motivate and retain health workers.
Motivation Project Goal and Objectives
The goal of the Motivation Project was to strengthen the evidence base for effective human resource strategies in developing countries. The project explored current capacities and contexts in three countries (Malawi, South Africa and Tanzania), evaluated local and national retention initiatives and explored in detail motivation and aspirations of health workers.
The objectives of the study were:
- To understand better the incentive and motivation environment facing health workers in district health service settings
- To assess the impact and relative importance of incentive initiatives that aim to improve recruitment, motivation and retention of health workers
- To improve the understanding of the absolute and relative power of financial and other incentives for different cadre levels
The systematic review of the literature indentified seven motivational themes, namely: financial rewards, career development, continuing education, hospital infrastructure, availability of resources and recognition/appreciation. While these factors are undoubtedly country specific, financial incentives, career development and management issues were core factors. Nevertheless financial incentives alone are not enough to improve morale.
Component Two evaluated financial and non-financial initiatives that are being used to motivate and retain health workers. Several themes emerged across the countries and it is apparent that while financial incentives do boost motivation to a certain extent, these effects are short lived and they also lower morale for those who do not benefit. In some countries there are lots of different incentives, many of which are not complimentary and so there is a strong case for consolidation and harmonization with close attention to monitoring and evaluating the effects.
Finally a discrete choice experiment (DCE) was used to improve understanding of the relative power of financial and non-financial incentives. It was found that the relative importance of different motivational incentives differs between countries; however, training opportunities and salary are the most important overall. Doctors and registered nurses are less motivated to work in rural areas.
All three components reinforced four main findings, namely:
1) Developing training opportunities would be a powerful motivational incentive.
2) Satisfied health workers are less motivated by financial incentives
3) Health workers, especially the higher cadres, may need to be compensated to persuade them to work in rural areas.
4) Clear communication and careful implementation is needed when using incentives so as to manage expectations.
Collaborating Partners
- Department of Community Health, College of Medicine, University of Malawi, Blanytre
- Centre for Health Policy, University of the Witwatersrand, Johannesburg
- National Institute for Medical Research (NIMR), Dar es Salaam
- Department of Epidemiology and Preventive Medicine, Royal College of Surgeons, Dublin
The Research Team
Prof. Charles Normand |
Trinity Centre for Global Health and Health Policy & Management, TCD |
Dr Eilish McAuliffe |
Trinity Centre for Global Health, TCD |
Prof. Malcolm MacLachlan |
Trinity Centre for Global Health and School of Psychology, TCD |
Dr. Steve Thomas |
Trinity Centre for Global Health and Health Policy & Management, TCD |
Posy Bidwell |
Trinity Centre for Global Health, TCD |
Prof. Ruairi Brugha |
Dept of Epidemiology & Public Health Medicine, Royal College of Surgeons |
Prof. Cameron Bowie |
Dept of Community Health, University of Malawi |
Duane Blaauw |
Centre for Health Policy, University of the Witwatersrand |
Dr. Aziza Mwisongo |
National Institute for Medical Research, Dar es Salaam |
The Motivation Project was led by Prof. Charles Normand, Principal Investigator