Welcome to this course on the use of cerebrospinal fluid (CSF) biomarkers in the diagnosis of Alzheimer's disease (AD). Since CSF biomarkers increase AD diagnostic certainty and can lead to earlier diagnosis, the course aims to improve the acceptance of the use of CSF biomarkers in AD diagnosis and to help standardise their use.
You may wish to view the course in its entirety or to view only the pages that are directly relevant to you.
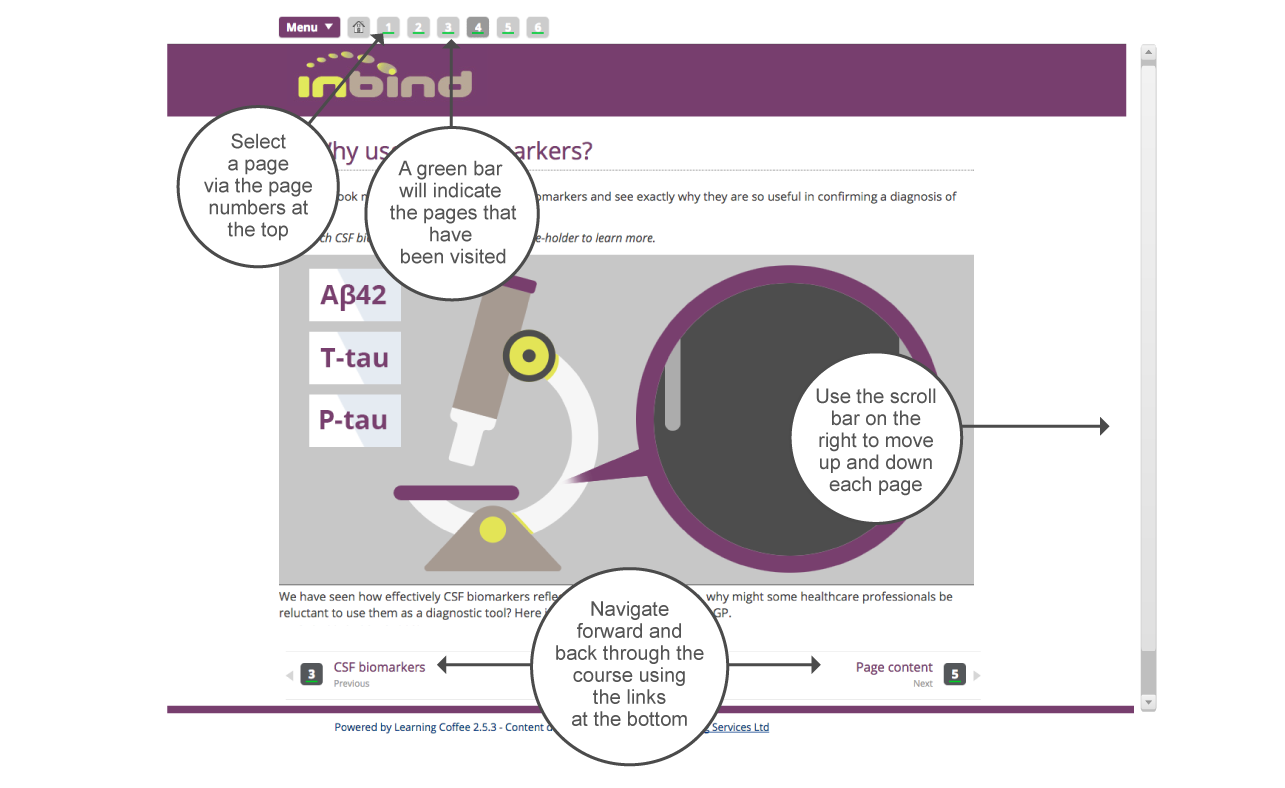
The annotated diagram below shows you how to navigate the course.
2.
Dementias: their human cost
We will look at the diagnostic use of CSF biomarkers, which have been shown to perform well in identifying AD, even in the disease’s early phase.
Dementias affect so many people worldwide that they entail huge economic and societal costs. According to World Health Organisation figures, 47 million people worldwide are affected, costing the global economy 1% of total GDP.
At a personal level, dementias such as AD exact a heavy human toll. We will be following the story of Sarah, a 52-year-old administrator, who has been displaying possible symptoms of the disease.
Click through all five slides below to read Sarah's story.
Sarah’s fears for her health mirror the fears of many of us as we grow older – though not usually at such a relatively young age as hers. She is aware of experiencing both a loss of memory and a decline in her ability to ‘think straight’ – i.e. process thoughts correctly. Might this indicate the kind of cognitive impairment characteristic of AD? And how might her doctor and his fellow health professionals come to a firm conclusion about that?
3.
What are CSF biomarkers?
Since dementia has various types and subtypes, and since there can be overlapping symptoms and also mixed forms of dementia, diagnosis can be difficult. This makes it all the more important that we discover definitive markers of these diseases and their progression – and that, when we do discover such markers, health professionals know how to use them.
What is a biomarker?
A biomarker is a measurable substance or activity which functions as a marker of a particular biological activity. Biomarkers can provide information on the status or progression of a disease, and can help measure the efficacy of treatment. Their use also extends to the areas of drug development, toxicity profiling and clinical trial screening.
Just how useful a biomarker is for diagnosis depends on its sensitivity and specificity for a particular disease.
A good biomarker:
Click the image to learn more.
Why use CSF biomarkers?
What would make the perfect biomarker for AD? Ideally, it would:
Click the arrow.
Since, as its name suggests, cerebrospinal fluid (CSF) bathes the brain and spinal cord, AD biomarkers are at their most concentrated in CSF. As well as CSF being relatively easy to access, by means of a lumbar puncture (LP), its composition reflects the metabolic processes associated with AD.
Previously, AD could only be discriminated from other dementias by a clinical assessment or a post mortem. But then three CSF biomarkers were developed for the different pathogenic processes of the disease. Their effectiveness is such that the clinical diagnostic criteria for AD dementia has been revised to include CSF biomarkers.
How effective are they? To take just one example: the inclusion of biomarker evidence in a memory clinic setting altered 10% of diagnoses and significantly increased clinician confidence in their diagnosis in 30% of cases.
What are the three CSF biomarkers?
The three core CSF biomarkers for AD are:
• Amyloid-beta42 (Aβ42)
• Phosphorylated tau (p-Tau)
• Total tau (t-Tau)
All three biomarkers are significantly altered in the CSF of AD patients, and reflect the pathophysiology associated with the disease. What is the nature of that pathophysiology? In essence, it has three aspects, as shown:
Slide the button along to reveal AD's pathophysiology as reflected by changes to the CSF biomarkers.
Let’s consider these three biomarkers for AD in the context of the characteristics of the disease.
Click the arrow buttons to learn more.
4.
Why use CSF biomarkers?
Now we’ll look more closely at the three CSF biomarkers and see exactly why they are so useful in confirming a diagnosis of AD.
Drag each CSF biomarker to the microscope's slide-holder to learn more. (If you would like to see the references, then click the highlighted words within the texts that appear.)
We have seen how effectively CSF biomarkers reflect the pathology of AD. So, why might some healthcare professionals be reluctant to use them as a diagnostic tool? Here is one typical response.
Such doubts are understandable. A lumbar puncture for a vulnerable patient might seem too invasive when the reality is that there is, as yet, no cure for AD. So how might practitioners be reassured enough to at least consider the procedure as an option?
Three points worth pondering are that:
Click the image.
Benefits to the patient and carer
Pathological biomarker levels can be observed as early as 10 years prior to the onset of clinical symptoms of AD. Yet, in the absence of a cure, what benefits could early diagnosis bring? Well, the sooner the diagnosis, the sooner the provision of:
Click through each of the five slides.
Diagnosing AD in its early stages should usher in the sort of treatment and support that would improve cognitive performance, delay or prevent institutionalisation, reduce carer stress, and improve carer and patient quality of life.
It’s now known that a diagnosis of dementia due to AD pathological processes can be made more certain by the inclusion of biomarker data. In one study involving individuals with mild cognitive impairment (MCI), CSF biomarkers displayed a sensitivity of 95% and specificity of 83% for detection of incipient AD in individuals with mild cognitive impairment.
5.
When to use CSF biomarkers
So, using CSF biomarkers can make certain of an AD diagnosis, but this doesn’t mean that their use is recommended in all cases. As with other aids to diagnosis, CSF biomarker results should be applied within the context of an individual’s entire clinical presentation. Consensus papers recommend that CSF biomarker analysis should be used in three main cases of cognitive impairment:
Click through the three slides.
In Sarah’s case
Sarah’s dementia specialist recommended that she undergo neuropsychological testing and brain imaging. The results of these have come back, and now he must decide if further investigation is required. Here are the results that will help him make that decision:
Click the highlighted terms in the table for more information.
Sarah’s neuropsychological profile is indicative of rapid forgetfulness. With inconclusive MRI/PET results and no evidence of functional impairment, and given Sarah’s relatively young age and family history of early onset AD, her dementia specialist suspects that she too could have mild AD dementia.
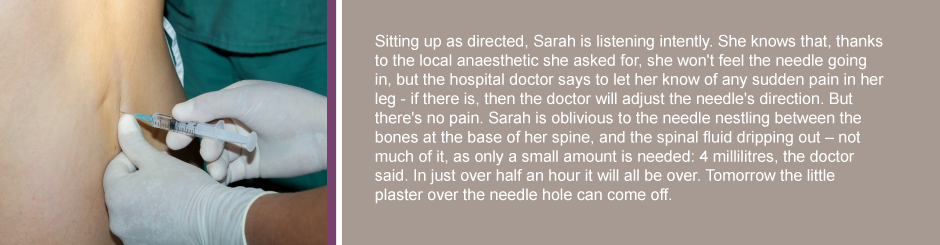
Knowing that CSF biomarker analysis might bring greater clarity, he is now going to recommend a LP. This will be performed at her local hospital.
It's vital to bear in mind that anyone about to undergo a CSF biomarker test has a cognitive impairment and may have dementia. This person needs to understand what is going on, so practitioners should explain clearly and provide written information on the benefits and risks of the procedure and test results in a way that is easily understood.
Prior to CSF biomarker testing, a person with cognitive impairment and their caregiver must be made aware that:
Click each coloured jigsaw piece.
Expectations
It's important that clinicians manage expectations by explaining that the test results may not lead to a definite diagnosis. And when it comes to disclosure, the wishes of each person undergoing the test should be respected: some may want full disclosure, while others may want to be told in less detail.
Click the carer on the left and the patient on the right to see the proportions of carers and patients who wish to have disclosure.
Sarah's CSF should be collected, processed and analysed just like everyone else's. As part of the drive to standardise CSF biomarker acquisition, processing and analysis, certain procedures for collecting CSF should be followed.
Click the purple circle to start. Click each of the coloured circles that subsequently appear.
Processing and storing
The acceptance of CSF biomarkers as AD diagnostic supports has been hampered by the degree of inter-assay and inter-laboratory variation – around 30% in some cases. One particular source of variation is the disparity in pre-analytical methodologies used by clinical and research laboratories to process and store CSF prior to analysis. Multi-centre quality control programmes and the adoption of universal standard operating procedures should go a long way towards addressing these issues and improving normalisation and comparison.
The following five procedures should always be followed.
Click each number.
Knowledge check
Let's see how much you were able to take in with this quick quiz.
Choose your answer then click Submit. Use the forward arrow to move to the next question.
7.
Interpreting the results
In most cases, CSF biomarkers aren't needed to support a diagnosis of AD. Where they are used, they can help determine whether clinical presentations are:
of 'high likelihood’ of being due to AD (i.e. Aβ42, t-Tau and p-Tau are abnormal)
of ‘intermediate likelihood’ of being due to AD (if only one type of biomarker evidence is apparent)
CSF biomarker results can fall into one of three categories – clearly positive, clearly negative or uninformative. To rule out AD, all three of the core CSF biomarkers (Aβ42, and t-Tau and p-Tau) must be in the normal range (reference ranges should be developed by each clinical/research centre). This would mean that the CSF biomarker profile is ‘neurochemically incompatible’ with AD.
If all three biomarkers are abnormal, then the CSF biomarker profile can be considered ‘neurochemically compatible’ with a CSF biomarker diagnosis of AD.
The diagnostic guidelines of the National Institute on Aging-Alzheimer’s Association outline the likelihood that a clinical presentation of dementia is due to AD – this likelihood can be supported by biomarker evidence.
Click Continue to see more information in the table.
Adapted from: McKhann et al., Alzheimers Dement (2011) 7: 263-269.
Impact of disclosure
Sarah's results have come back from the lab as follows:
Biomarker
Normal Cut Off Conc. (pg/mL)
Test Result
CSF Aβ42 (pg/mL):
normal conc. > 550
400 pg/mL
CSF t-Tau (pg/mL):
normal range: 146–385
500 pg/mL
CSF p-Tau (pg/mL):
normal range: 24–68
78 pg/mL
Her dementia specialist must consider these CSF biomarker results in conjunction with the clinical, MRI/PET and neuropsychological results. The diagnosis he forms on the basis of all of these is that Sarah has a mild cognitive impairment due to underlying AD pathology.
Understandably, the news comes as a tremendous shock to Sarah, and her reaction is not uncommon. However, aprospective evaluation of the impact of disclosure on patient and carer anxiety and depression revealed a reduction in anxiety levels and no change in depression scores in those assessed three days after evaluation. Both carers and patients have reported that disclosure allows them to make appropriate provision for their future. Carers have indicated that they wish they had known the diagnosis earlier so that they could have adapted better and made changes sooner.
8.
Case study 1: Hao
Putting your knowledge into practice
Now that you have a better idea of when it may be clinically advised to use CSF biomarker analysis and what the results of such an analysis may signify, see what conclusions you would come to in the case studies presented on this page and the next.
Hao is a retired professional, 67 years old, who presents with a two-year history of gradually worsening forgetfulness.
Click Play to find out more, and then click Continue.
9.
Case study 2: Billy
Now consider the case of Billy, a 76-year-old former mechanic who presents with a one-year history of word-finding difficulties.
Click Play to find out more, and then click Continue.
10.
Key points
You have now completed this course on the use of CSF biomarkers in AD diagnosis. A pdf of resources and references can be downloaded here. The following are some of the key points to take from the course:
Click the cogs as they appear.
Simply close the browser tab to exit the course.
clinical diagnostic criteria
McKhann et al., Alzheimer Dement (2011) 7:263-269; Dubois et al., Lancet Neurol (2007) 6: 734-746; Dubois et al., Lancet Neurol (2014) 13: 614-629
memory clinic setting
Kester et al., Dement Geriatr Cogn Disord (2010) 29: 491-497
prospective evaluation
Carpenter BD et al. J Am Geriatr Soc (2008) 56(3):405-412.
indicated
Connell CM et al. Gerontologist (2004) 44(4):500-507.
reported
Derksen E et al. Aging Ment Health (2006); 10(5):525-531.
MMSE
The Mini Mental State Examination (MMSE) is a 30-point questionnaire which examines functions including registration, attention and calculation, recall, language and orientation; a score >24 is considered in the normal range; 20-24 mild dementia; 13-20 moderate dementia, and <13 severe dementia
CAMCOG-R
The Cambridge Cognitive Examination Revised (CAMCOG-R) is designed to assess the extent of impairment in several cognitive domains, including orientation, language, memory, praxis, attention, abstract thinking, perception and calculation. It is scored out of a total of 105; a score >80 is normal.
RBANS
The Repeatable Battery for Assessment of Neurological Status (RBANS) consists of ten subtests which give five scores, one for each of the five domains tested (immediate memory, visuospatial/constructional, language, attention, delayed memory). Index average = 100 ± 15 = 1 Std Dev. PR = Percentile.
MoCA
The Montreal Cognitive Assessment (MoCA) screening tool is a test for cognitive impairment. With a combined total of 30 points, it assesses several domains: Delayed recall (5 points); Visuospatial/executive (5 points); Naming (3 points); Attention (6 points); Language (3 points); Abstraction (2 points); and Orientation (6 points). A score >25 is normal.
CDR
Clinical Dementia Rating (CDR) is a numeric scale used to assess the severity of symptoms of dementia. It scores an individual’s cognitive and functional performance in six areas: memory, orientation, judgement and problem solving, community affairs, home and hobbies, and personal care. It is scored 0–3; a score of 0 is none; a score of 0.5 is suspect; a score of 1 is mild; a score of 2 is moderate; a score of 3 is severe.
MRI
Magnetic resonance imaging (MRI) is a technique that uses a magnetic field and radio waves to create detailed images of the organs and tissues within the body.
FDG-PET
A positron emission tomography (PET) scan is an imaging test that helps reveal how the body’s tissues and organs are functioning. A fluorodeoxyglucose–positron emission tomography (FDG-PET) scan of the brain measures regional glucose use and can be used to differentiate AD from other dementias, and also to make early diagnosis of AD.
Drugs - When do they work?
Current pharmacological therapies for AD address the symptoms of the disease, but do not treat the disease or delay progression. At present, CSF biomarker testing is used in clinical settings primarily to increase the confidence of a diagnosis of AD. However, if current clinical trials of disease-modifying drug candidates are successful, the diagnostic use of CSF biomarkers could increase dramatically, as there will be a need for earlier and more accurate diagnosis to allow treatment at the pre-dementia and potentially the pre-symptomatic stages of AD.
one study
Hansson et al., Lancet Neurol (2006) 5: 228-234
neurochemically incompatible
Molinuevo et al., (2014) Alzheimer Dement 10: 808-817.
statistics reference
Pinner at al., (2003) Int Psychogeriatr15(3):279-288
around 30% in some cases
Mattsson et al., (2013) Alzheimer Dement 9: 251 – 261